ALLERGY: How? Who? What? When? and Which?
Allergy is a hypersensitivity disorder of the immune system, where our body hyper reacts to a normally harmless substance; one that does not bother most people. People who have allergies are often sensitive to more than one substance. Going by that definition any substance is a potential allergen.
Allergy is a Type I hypersensitivity reaction, immunologic in nature, occurring within minutes after the combination of antigen and antibody bound to a mast cell in an individual previously sensitized to the antigen. It could be a systemic or localized reaction depending on the antigen (allergen) involved.
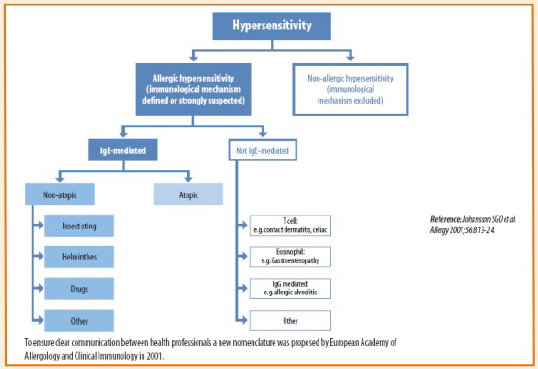
Most allergic hypersensitive reactions are a topic in nature.
Atopy is a personal and/or familial tendency, usually in childhood or adolescence, to become sensitized and produce IgE antibodies in response to ordinary exposure to allergens, usually proteins. As a consequence these individuals can develop typical symptoms of asthma, rhino conjunctivitis or eczema.
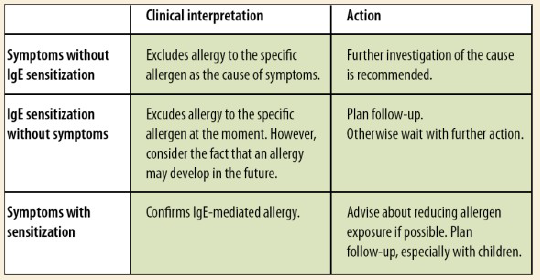
Allergen exposure is a prerequisite for sensitization in a topic individuals. IgE antibodies can be detected very early in the blood, even before symptoms become evident; hence IgE sensitization is a “risk marker” for developing allergy.

So the million dollar question that arises is WHY do we need to test for allergy?
As doctors and patients alike will tell you, most allergies share common symptoms. Food allergies start with nausea, vomiting, diarrhea, pain abdomen or a skin rash. Dermatological allergies present with dermatitis and urticaria. Respiratory ailments present with rhinitis or wheeze. Also rarely there is a potential chance of an anaphylactic reaction that could be life threatening. That is why testing for allergies as a separate entity not only helps categorize patient as allergic or non- allergic but further their referral for optimal treatment is possible.
Secondly; indiscriminate use of anti histamines and antibiotics leads to a heavy burden on health costs, when they are prescribed to patients with “allergy like symptoms.” A correct diagnosis could minimize the misuse to a great extent.
Thirdly and most pertinently when medical history is not sufficient for pinpointing the poly sensitized nature of the patient it is imperative to find out the offending allergens as combined sensitization can act in unison to cause an overt illness.
WHO do we test?
• All patients with recurrent or persistent “allergy-like” respiratory, skin and gastro symptoms
• Blocked or runny nose
• Nasal catarrh
• Itchy runny eyes
• Cough
• Breathing difficulties
• Dry itchy skin
• Diarrhea
• Stomach pains
• Or patients with uncontrolled allergy disease.
Patients with allergies have a tendency to develop newer allergies over a period of time. This is called allergy march. Testing regularly to a get a true and actual picture of current exposure can help the patient avoid that particular allergen.

When will the symptoms appear?
This tends to vary between individuals as it would depend upon:
— The degree of exposure
— The level of IgE antibodies
— Degree of atopy
— The individual’s clinical reactivity
The obvious corollary to the Whys, who and when to test is which allergen should we be testing for? Although clinical history might be leading in some case, few guidelines could be of much use in deciding.
• The individual exposure will dictate the allergens to test
• Some allergens are more common than others
• Additional parameters to consider are:
— Age
— Symptoms
— Environment (pets, hobbies, work etc.)
— Geographic living
Also to keep in mind that fewer allergens are responsible for majority of allergies, hence look for the local most common allergens first before moving on to the rarer ones.
ALLEGY TESTING
Immunocap is a Fluorescent enzyme immunoassay which is by far the gold standard in in-vitro allergy testing world wide.
It can be performed irrespective of:
— Age
— Symptom
— Disease activity/or severity
— Antihistamine medication
— Pregnancy
It also provides allergen level as low as 0.1KAU/L which is approved by US FDA and is traceable to W. H.0 standard.
Recommended testing protocol:
Step 1: Phadiatop: it is a qualitative test to distinguish between atopic and non-atopic individual.
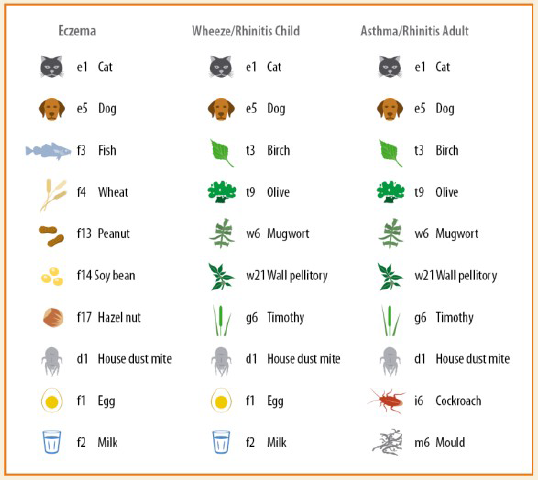
Step 2: Symptom profiles (fixed allergen panels)
– Identify allergic patients
Step 3: Follow-up testing
Explore other causative allergens
• Alternatively a Comprehensive allergy panel which includes
— Phadiatop
— Total IgE levels
— 32 specific IgE allergens
In short – Immunocap testing results:
• Show patients’ baseline IgE antibody levels
• Evaluate which allergens are the most probable for causing symptoms
• Evaluate if specific immunotherapy (SIT) is an option
• Follow changes over time to:
— reflect the effect of and compliance with allergen avoidance/reduction
— optimize medical strategies
— evaluate tolerance development (food allergy, SIT)
— avoid unnecessary food challenges
At Dr. Lal Pathlabs we are providing various panels in allergy testing depending on the patient symptom profile and doctors requirement.
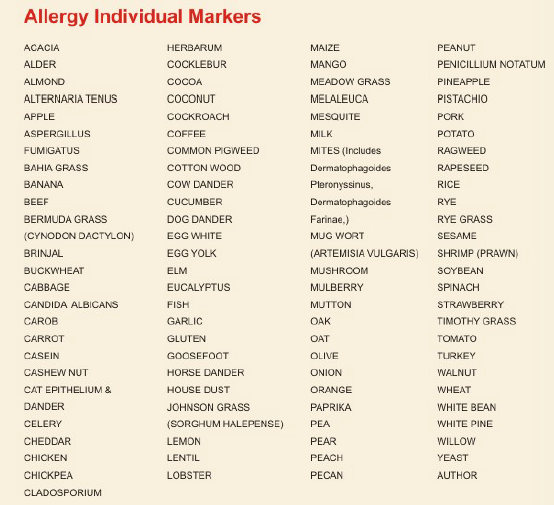
Includes Allergy Screening, Panels & Individual allergens
Other Allergy Profile/Panels
ALLERGY, ANIMALPANEL (Includes Cat epithelium. Cow. Dog and Horse Dander)
ALLERGY, ANIMALPANEL (Includes Oat, Maize, Sesame, Buckwheat, Rye. Wheat ,Rice and Carob)
ALLERGY, DUST PANEL (Includes House dust, Mites like Dermatophagolds Pteronyssinus, Dermatophagolds Farinae & Cockroach)
ALLERGY, ECZEMA PANEL (Includes Egg white, Cow’s Milk, Fish, Shrimp, Wheat. Rice. Peanut Lentil. Soybeans, Chick Pea. Lemon, Banana Mites, Dog dander, Cow dander, Horse dander and cat epithelium)
ALLERGY, FOOD PANEL (Includes Egg White Milk, Wheat Soybean, Fish, Chicken, Rice, Gluten, Shrimp and Peanut
ALLERGY, FRUIT PANEL (Includes Orange. Apple. Banana. Peach. Mango. Strawberry. Pear. Lemon. Pineapple and Coconut)
ALLERGY, GRASS PANEL (Includes Bermuda grass, Ray grass. Timothy grass. Meadow grass. Johan grass. and Bahia grass)
ALLERGY, MOLD PANEL (Includes Pericillium notatum, Cladosporium herbarum, Aspergillus fumigatus, Candida albicans and Alternaria tenuis)
ALLERGY, NON VEGETARIAN PANEL (Includes Pork, Beef, Egg yolk, Turkey, Mutton Lobster, Chicken, Fish, Shrimp and Egg white)
ALLERGY, NUT PANEL (Includes pecan, Cashew nut, Pistachio, Walnut, Almond and Peanut)
ALLERGY, PULSES PANEL (Includes Lentils, White bean and Chick pea)
ALLERGY, TREE PANEL (Includes Acacia, Olive, Willow, Melaieuca, White pine and Eucalyptus)
ALLERGY, TREE PANEL EXTENDED (Includes Olive, Willow, Melaieuca, White pine and Eucalyptus Acacia, Elm, Alder, Oak, Cottonwood, Mesquite and Mulberry)
ALLERGY, VEGETABLE PANEL (Includes Spinach, Cabbage, Paprika, Tomato, Mushroom, Garlic, Onion, Celery, Carrot, Potato, Cucumber and Brinjal)
ALLERGY, WEED PANEL (Includes Pagweed, Goosefoot, Common pigweed, Coklebur, Mugwort and Rapeseed)
ALLERGY, WHEEZE / RHINITIS PANEL, ADULT (Includes Elm, Bermuda grass, Rye grass, Timothy grass, Meadow grass, Johnson grass, Bahia grass, Alder, Mugwort, Common pigweed, Gluten, Pea, Casein, House dust Cocoa, Coffee, Cheddar, Mesquite, Ragweed, Goosefoot, Cat epithelium, Dog dander Cockroach, Alterneria tenuis, Aspergillus fumigatus, Candida albicans, Penicillium notatum and cladosporium herbarum)
ALLERGY, WHEEZE / RHINITIS PANEL, PEDIATRIC (Includes Elm, Mesquite Ragweed, Goosefoot, Egg white, Milk, Rice, Lentil, Pea, White bean, Cat epithelium, Dog dander Mites, Cockroach, Lemon, Alterneria tenuis, Aspergillus fumigatus, Candida albicans, Penicillium notatum and Cladosporium herbarum)
ALLERGY, SCREEN (Includes Total IgE and Phadia Top) ALLERGY, POST SCREENING PROFILE (Includes Allergy Panels & Individual allergens)
ALLERGY, COMPREHENSIVE PROFILE (Includes Allergy Screening, Allergy Panels & Individual allergens)
ANY 5/10 ALLERGENS
Dr. Sushrut Pownikar
Head of Department
Hematology & Sp. Immunology
Dr. Lal PathLabs Pvt Ltd
 From the Editor’s desk
From the Editor’s desk
Growing industrialisation and fast changing biodiversity coupled with sedentary lifestyles are causing a surge in allergic diseases, especially among children in the country. Currently, about 20 to 30 per cent of people in India are having one or more allergic diseases and their prevalence is rising dramatically. Allergies have a major impact on quality of life and work productivity and thus affects the socio-economic fabric of the country,
The diseases included asthma, rhinitis, anaphylaxis, food and drug allergy, insect allergy, eczema and urticaria (hives) and angioedema.
The prevalence of asthma and rhinitis – two major forms of allergies -was one and 10 percent respectively in 1964 in the country. But, new data shows that about 14 per cent people now have asthma, while over 20 per cent are suffering from allergic rhinitis (AR) which results from an IgE-mediated inflammation of the nasal mucosa.
This increase is especially affecting children, who are bearing the greatest burden of the rising trend which has occurred over the last two decades.
Reasons behind this surge are multiple – growing pollution due to urbanisation, rising temperature and change in lifestyle. Environmental changes are affecting pollen counts, while prevalence of molds linked with allergic diseases and sedentary lifestyles weakens the immune system, increasing ones susceptibility to allergies. Over-hygienic lifestyles also drive the rise in allergies and asthma. Insulated spaces are also a veritable breeding ground for allergies and could lead to a complete deterioration of the indoor air quality, further stressing the need to keep indoors well-ventilated.
Anyone with allergies should ask the question: “why do I have allergies?” Allergies are the sign of dysfunction in the body and allergies are not normal. Most people spend their time and money treating the allergy symptoms while the causes go untreated. Controlling the disease by increasing awareness and appropriate evidence-based treatment is crucial.
In this issue, Dr Sushrut Pownikar, covers the range of tests available to detect and categorize these allergic disorders for further prevention and treatment. He answers the common questionsHow? Who? What? When? and Which? ofAllergic disorders.
Your appreciative feedback is very encouraging and we look forward to suggestions to help us improve and provide you the best quality information in the field of diagnostic test and their application in clinical diagnosis and treatment. We look forward to your participation and continued support.